This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs".
This E log book also reflects my patient-centred online learning portfolio and your valuable comments on comment box is welcome.
 ESR : ELEVATED
ESR : ELEVATED

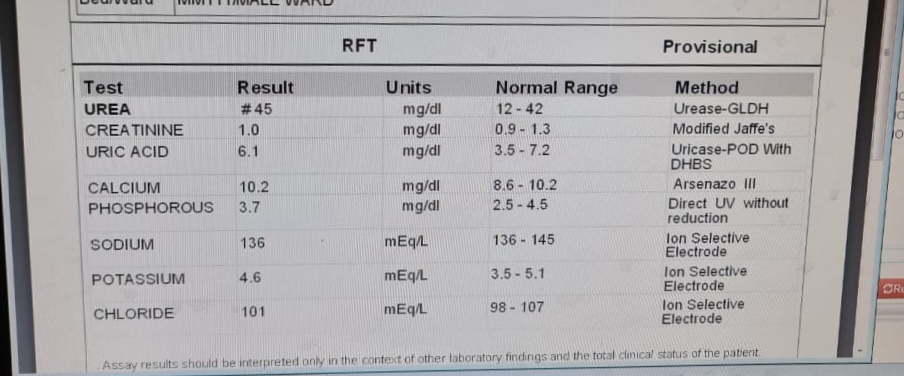
RFT: ELEVATED UREA
 D DIMER
D DIMER

LFT: ELEVATED ALP



Name : Kattekola Sathwik
Roll no: 58
8th semester
Following details were provided to me by Intern Dr Anjali ma'am.
Case details
A 45 year old male has presented with the casuality with the chief complaints of sudden onset shortness of breath on 2nd June 2021
History of presenting illness
The patient was apparently asymptomatic till June 2nd .
Then he developed grade 4 SOB which is of sudden onset.
There was a history of orthopnea
No history of fever, cough, cold, sore throat, loss of appetite, chest pain, palpitations, giddiness, sweating, blurring of visions, blackout
Based on the above history he was sent for rapid antigen test for covid-19 which he was tested positive on 2nd June 2021 and then he was admitted in COVID ICU
History of past illness
No history of diabetes hypertension tuberculosis or epilepsy
Personal history
Appetite : normal
Diet : mixed
Bowel and bladder habits: regular
Sleep : adequate
Addictions: No addictions
No history of drug and food allergies
Family history: not significant
General examination
The patient is conscious for rent in cooperative
He is well oriented to time place and person
Moderately built and moderately nourished
Pallor: absent
Icterus:absent
Cyanosis:abent
Clubbing:absent
Lymphadenopathy: absent
Edema: absent
Vitals
Temperature: afebrle
Pulse: 132bpm
Respiratory rate:33cpm
Blood pressure: 90/60 mmHg
SPO2:91 on room air
GRBS:100mg%
Systemic examination:
Cardiovascular system: s1 s2 heard, No thrills and murmurs
Respiratory system;
- DYSPNEA ; PRESENT
- BILATERAL CREPTS
Abdomen: SOFT and NON TENDER
CNS: NAD
Provisional diagnosis: VIRAL PNEUMONIA SECONDARY TO COVID -19
Investigations
HEMOGRAM: INCREASE IN NEUTROPHILS.


RFT: ELEVATED UREA

LFT: ELEVATED ALP

HRCT THORAX



| TREATMENT : |
ON 2ND JUNE 2021
- NEB. BUDECORT+DUOLIN 8TH HOURLY
- TAB. PARACETAMOL500mg PO/SOS
- TAB.PANTOP 40mg PO/OD
- TAB.LIMCEE OD
- TAB.ZINCOVIT OD
- O2 SUPPLEMENTATION @10L/MIN MAINTAINING AT SPO2 92%
- CONTINUOUS MONITORING OF BP ,SPO2 AND GRBS
- O2 SUPPLEMENTATION TO MAINTAIN SPO2 >92%
- TAB.PCM 650MG PO SOS
- TAB PANTOP 40 MG PO OD\TAB. LIMCEE PO OD
- TAB MVT PO OD
- NEB. WITH DUOLIN +BUDECORT 8TH HOURLY
- TAB. AUGMENTIN 625MG /PO/BD
- CONTINUOUS MONITORING
- O2 SUPPLEMENTATION
- TAB AUGMENTIN 625MG BD
- TAB LIMCEE OD
- TAB ZINCOVIT OD
- TAB PANTOP 40 MG OD
- TAB DOLO 650 MG BD
- NEBULIZATION WITH DUOLIN +BUDECORT 8TH HOURLY
I thank Dr Anjali ( intern) ma'am, Dr Vinay sir for helping me to make this log and I thank Dr Rakesh sir for this opportunity.
Comments
Post a Comment